Also see:
Endotoxin: Poisoning from the Inside Out
Protection from Endotoxin
Endotoxin-lipoprotein Hypothesis
Low Sodium Diet: High FFA, Insulin Resistance
Aldosterone, Sodium Deficiency, and Insulin Resistance
The Randle Cycle
Free Fatty Acids Suppress Cellular Respiration
Dairy, Calcium, and Weight Management in Adults and Management
Belly Fat, Cortisol, and Stress
Stress and Aging: The Glucocorticoid Cascade Hypothesis
TNF-alpha and insulin resistance:
Trends Endocrinol Metab. 2000 Aug;11(6):212-7.
Potential role of TNF-alpha in the pathogenesis of insulin resistance and type 2 diabetes.d
Moller DE.
Tumor necrosis factor alpha (TNF-alpha) has well-described effects on lipid metabolism in the context of acute inflammation, as in sepsis. Recently, increased TNF-alpha production has been observed in adipose tissue derived from obese rodents or human subjects and TNF-alpha has been implicated as a causative factor in obesity-associated insulin resistance and the pathogenesis of type 2 diabetes. Thus, current evidence suggests that administration of exogenous TNF-alpha to animals can induce insulin resistance, whereas neutralization of TNF-alpha can improve insulin sensitivity. Importantly, results from knockout mice deficient in TNF-alpha or its receptors have suggested that TNF-alpha has a role in regulating in vivo insulin sensitivity. However, the absence of TNF-alpha action might only partially protect against obesity-induced insulin resistance in mice. Multiple mechanisms have been suggested to account for these metabolic effects of TNF-alpha. These include the downregulation of genes that are required for normal insulin action, direct effects on insulin signaling, induction of elevated free fatty acids via stimulation of lipolysis, and negative regulation of PPAR gamma, an important insulin-sensitizing nuclear receptor. Although current evidence suggests that neutralizing TNF-alpha in type 2 diabetic subjects is not sufficient to cause metabolic improvement, it is still probable that TNF-alpha is a contributing factor in common metabolic disturbances such as insulin resistance and dyslipidemia.
Nature. 1997 Oct 9;389(6651):610-4.
Protection from obesity-induced insulin resistance in mice lacking TNF-alpha function.
Uysal KT, Wiesbrock SM, Marino MW, Hotamisligil GS.
Obesity is highly associated with insulin resistance and is the biggest risk factor for non-insulin-dependent diabetes mellitus. The molecular basis of this common syndrome, however, is poorly understood. It has been suggested that tumour necrosis factor (TNF)-alpha is a candidate mediator of insulin resistance in obesity, as it is overexpressed in the adipose tissues of rodents and humans and it blocks the action of insulin in cultured cells and whole animals. To investigate the role of TNF-alpha in obesity and insulin resistance, we have generated obese mice with a targeted null mutation in the gene encoding TNF-alpha and those encoding the two receptors for TNF-alpha. The absence of TNF-alpha resulted in significantly improved insulin sensitivity in both diet-induced obesity and that resulting for the ob/ob model of obesity. The TNFalpha-deficient obese mice had lower levels of circulating free fatty acids, and were protected from the obesity-related reduction in the insulin receptor signalling in muscle and fat tissues. These results indicate that TNF-alpha is an important mediator of insulin resistance in obesity through its effects on several important sites of insulin action.
Nihon Rinsho. 1999 Mar;57(3):622-6.
[Syndrome X].
Kotake H, Oikawa S.
Insulin resistance is an early and major feature in the development of non-insulin-dependent diabetes mellitus (NIDDM). It is also associated with hyperlipidemia, hypertension, obesity and cardiovascular disease. It is the clustor of the risk factors for atherosclerosis and recognized as ‘insulin-resistance syndrome’ (Syndrome X). Central (abdominal) obesity is much more strongly associated with insulin resistance than overall obesity. The increase of both the influx of free fatty acid to liver and the production of TNF-alpha in adipose tissue may play an important role in mechanism of insulin resistance associated with central obesity. Calorie restriction and weight loss improve insulin sensitivity in overweight humans. Exercise training also improves insulin sensitivity via increased oxidative enzymes, glucose transporters (GLUT4) and capillarity in muscle as well as by reducing abdominal fat. The new ‘glitazones’ (thiazolidinediones) is used clinically to improve insulin sensitivity.
Physiol Res. 1998;47(4):215-25.
Thiazolidinediones–tools for the research of metabolic syndrome X.
Komers R, Vrána A.
“The resistance to insulin (insulin resistance, IR) is a common feature and a possible link between such frequent disorders as non-insulin dependent diabetes mellitus (NIDDM), hypertension and obesity…Furthermore, TDs inhibit the pathophysiological effects exerted by tumour-necrosis factor (TNF alpha), a cytokine involved in the pathogenesis of IR [insulin resistance].”
Exp Clin Endocrinol Diabetes. 1999;107(2):119-25.
Mechanisms of TNF-alpha-induced insulin resistance.
Hotamisligil GS.
There is now substantial evidence linking TNF-alpha to the presentation of insulin resistance in humans, animals and in vitro systems. We explored the relationship between TNF-alpha and insulin resistance using knockout mice deficient for either TNF-alpha or one or both of its receptors, p55 and p75. In studies of TNF-alpha-deficient knockout mice with diet-induced obesity, obese TNF-alpha knockouts responded to an exogenous dose of insulin or glucose much more efficiently than TNF-alpha wild-type animals. This finding suggests that deletion of TNF-alpha leads to increased insulin sensitivity, ie decreased insulin resistance. In studies using genetically obese ob/ob mice, TNF-alpha receptor wild-type and p75 receptor knockout animals developed a pronounced hyperinsulinemia and transient hyperglycaemia, whereas p55 receptor and double-knockout animals did not. Moreover, in glucose and insulin tolerance tests, we found that p75 knockout animals exhibited profiles identical to those of the wild-type animals, but that p55 knockout animals and double mutants showed a mild improvement in insulin sensitivity, relative to the wild type. Since the improvement in sensitivity was slightly greater with double mutants, p55 alone cannot be responsible for TNF-alpha’s promotion of insulin resistance in obese mice, despite the likelihood that it is more important than p75. How TNF-alpha-related insulin resistance is mediated is not fully clear, although phosphorylation of serine residues on IRS-1 has previously been shown to be important. When we monitored Glut 4 expression in obese TNF-alpha wild-type and knockout mice, we found no convincing evidence that TNF-alpha mediation of the down-regulation of Glut 4 mRNA expression is responsible for insulin resistance. However, we found an approximately 2-fold increase in insulin-stimulated tyrosine phosphorylation of the insulin receptor in the muscle and adipose tissue of TNF-alpha knockout mice, suggesting that insulin receptor signalling is an important target for TNF-alpha. Other possible mediators of TNF-alpha-induced insulin resistance include circulating free fatty acids (FFAs) and leptin.
TNF-alpha and obesity:
The Journal of Clinical Endocrinology & Metabolism August 1, 1998 vol. 83 no. 8 2907-2910
Tumor Necrosis Factor-α in Sera of Obese Patients: Fall with Weight Loss
Paresh Dandona, Ruth Weinstock, Kuldip Thusu, Ehad Abdel-Rahman, Ahmad Aljada, and Thomas Wadden
In view of the recent demonstration that obesity in animals and humans is associated with an increase in tumor necrosis factor-α (TNFα) expression, that this expression falls with weight loss, and that TNFα may specifically inhibit insulin action, the possibility that TNFα may be a mediator of insulin resistance has been raised. We have undertaken this study to investigate whether serum TNFα concentrations are elevated in obese subjects, whether they fall after weight loss, and whether this fall parallels the fall in insulin release after glucose challenge. Obese patients (age range: 25–54, weight mean ± sd: 96.4 ± 13.8 kg, body mass index: 35.7 ± 5.6 kg/m2) were started on a diet program. The mean weight fell to 84.5 ± 11.3 (P < 0.0001) and body mass index to 31.3 ± 4.9 (P < 0.0001). Plasma TNFα concentrations were markedly elevated in the obese (3.45 ± 0.16 pg/mL), when compared with controls (0.72 ± 0.28 pg/mL), and fell significantly (2.63 ± 1.40 pg/mL) after weight loss (P < 0.02). The magnitude of insulin release after glucose (75 g) challenge (area under the curve) also fell significantly (P < 0.01) after weight loss. The magnitude of weight loss and fall in TNFα were related to basal body weight (r = 0.57, P < 0.001) and basal TNFα (r = 0.55, P < 0.001) concentrations, respectively, but not to each other or to the glucose-induced insulin release (area under the curve). We conclude that obesity is associated with increased plasma TNFα concentrations, which fall with weight loss. Because circulating TNFα may mediate insulin resistance in the obese, a fall in TNFα concentrations may contribute to the restoration of insulin resistance after weight loss, Thus, TNFα may be an important circulating cytokine, which may provide a potentially reversible mechanism for mediating insulin resistance.
Endotoxin Increases TNF-alpha, Associated with Insulin Resistance and Diabetes:
Diabetes Care February 2011 vol. 34 no. 2 392-397
Endotoxemia Is Associated With an Increased Risk of Incident Diabetes
Pirkko J. Pussinen, PHD1, Aki S. Havulinna, MSC2, Markku Lehto, PHD3,4, Jouko Sundvall, MSC2 and Veikko Salomaa, MD2
OBJECTIVE Diabetes is accompanied with a chronic low-grade inflammation, which may in part be mediated by endotoxins derived from Gram-negative bacteria.
RESEARCH DESIGN AND METHODS We investigated in a population-based cohort whether endotoxemia is associated with clinically incident diabetes. The serum endotoxin activity was measured by limulus assay from the FINRISK97 cohort comprising 7,169 subjects aged 25–74 years and followed up for 10 years.
RESULTS Both the subjects with prevalent diabetes (n = 537) and those with incident diabetes (n = 462) had higher endotoxin activity than the nondiabetic individuals (P < 0.001). The endotoxin activity was significantly associated with increased risk for incident diabetes with a hazard ratio 1.004 (95% CI 1.001–1.007; P = 0.019) per unit increase resulting in a 52% increased risk (P = 0.013) in the highest quartile compared with the lowest one. The association was independent of diabetes risk factors: serum lipids, γ-glutamyl transferase, C-reactive protein, BMI, and blood glucose. Furthermore, the association of endotoxemia with an increased risk of incident diabetes was independent of the metabolic syndrome as defined either by the National Cholesterol Educational Program-Adult Treatment Panel III or the International Diabetes Federation. Endotoxin activity was linearly related (P < 0.001) to the number of components of the metabolic syndrome.
CONCLUSIONS Both prevalent and incident diabetes were associated with endotoxemia, which may link metabolic disorders to inflammation. The results suggest that microbes play a role in the pathogenesis of diabetes.
Diabetes Care. 2011 Feb;34(2):392-7.
Endotoxemia is associated with an increased risk of incident diabetes.
Pussinen PJ, Havulinna AS, Lehto M, Sundvall J, Salomaa V.
Both prevalent and incident diabetes were associated with endotoxemia, which may link metabolic disorders to inflammation. The results suggest that microbes play a role in the pathogenesis of diabetes.
Diabetes. 2007;56(7):1161-1772.
Metabolic Endotoxemia Initiates Obesity and Insulin Resistance
Patrice D. Cani; Jacques Amar; Miguel Angel Iglesias; Marjorie Poggi; Claude Knauf; Delphine Bastelica; Audrey M. Neyrinck; Francesca Fava; Kieran M. Tuohy; Chantal Chabo; Aurélie Waget; Evelyne Delmée; Béatrice Cousin; Thierry Sulpice; Bernard Chamontin; Jean Ferrières; Jean-François Tanti; Glenn R. Gibson; Louis Casteilla; Nathalie M. Delzenne; Marie Christine Alessi; Rémy Burcelin
Diabetes and obesity are two metabolic diseases characterized by insulin resistance and a low-grade inflammation. Seeking an inflammatory factor causative of the onset of insulin resistance, obesity, and diabetes, we have identified bacterial lipopolysaccharide (LPS) as a triggering factor. We found that normal endotoxemia increased or decreased during the fed or fasted state, respectively, on a nutritional basis and that a 4-week high-fat diet chronically increased plasma LPS concentration two to three times, a threshold that we have defined as metabolic endotoxemia. Importantly, a high-fat diet increased the proportion of an LPS-containing microbiota in the gut. When metabolic endotoxemia was induced for 4 weeks in mice through continuous subcutaneous infusion of LPS, fasted glycemia and insulinemia and whole-body, liver, and adipose tissue weight gain were increased to a similar extent as in high-fat-fed mice. In addition, adipose tissue F4/80-positive cells and markers of inflammation, and liver triglyceride content, were increased. Furthermore, liver, but not whole-body, insulin resistance was detected in LPS-infused mice. CD14 mutant mice resisted most of the LPS and high-fat diet-induced features of metabolic diseases. This new finding demonstrates that metabolic endotoxemia dysregulates the inflammatory tone and triggers body weight gain and diabetes. We conclude that the LPS/CD14 system sets the tone of insulin sensitivity and the onset of diabetes and obesity. Lowering plasma LPS concentration could be a potent strategy for the control of metabolic diseases.
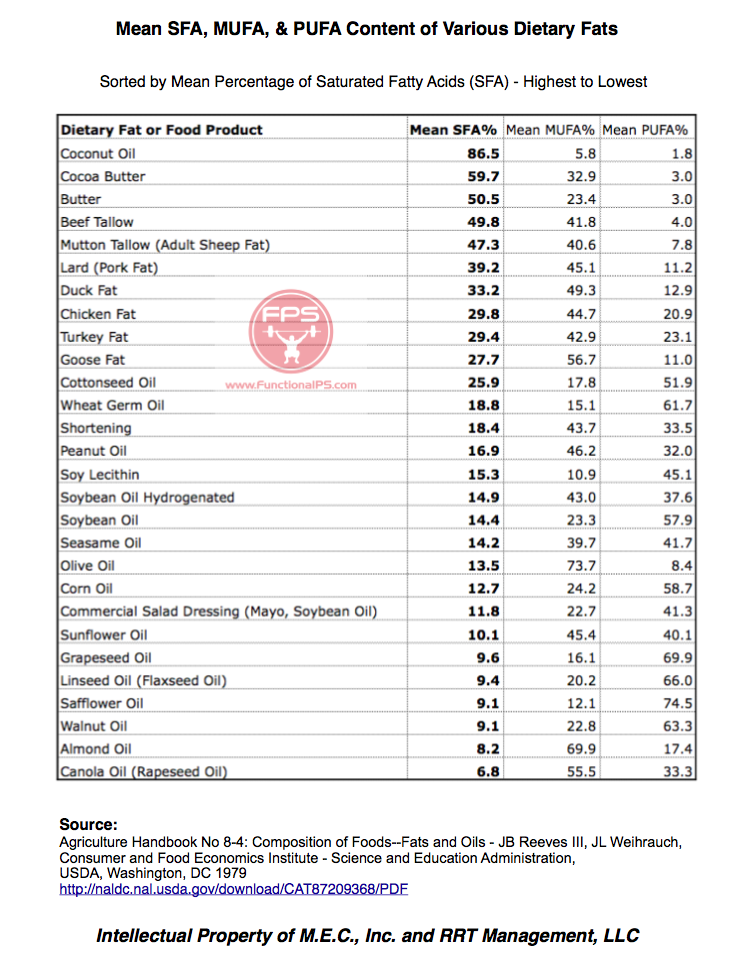
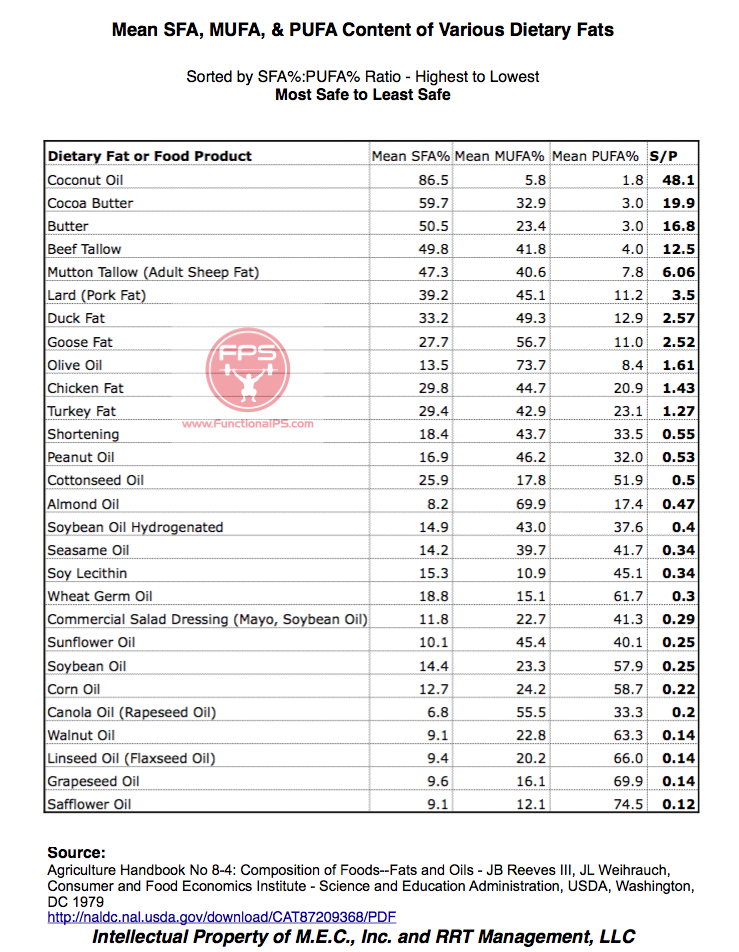
Saturated fats reduce endotoxemia, lipid peroxidation, and TNF-alpha:
Hepatology. 1997 Dec;26(6):1538-45.
Dietary saturated fatty acids down-regulate cyclooxygenase-2 and tumor necrosis factor alfa and reverse fibrosis in alcohol-induced liver disease in the rat.
Nanji AA, Zakim D, Rahemtulla A, Daly T, Miao L, Zhao S, Khwaja S, Tahan SR, Dannenberg AJ.
We investigated the potential of dietary saturated fatty acids to decrease endotoxemia and suppress expression of cyclooxygenase 2 (Cox-2) and tumor necrosis factor alpha (TNF-alpha) in established alcohol-induced liver injury. Six groups (five rats/group) of male Wistar rats were studied. Rats in group 1 were fed a fish oil-ethanol diet for 6 weeks. Rats in groups 2, 3, and 4 were fed fish oil and ethanol for 6 weeks. Ethanol administration was stopped at this time, and the rats were switched to isocaloric diets containing dextrose with fish oil (group 2), palm oil (group 3), or medium-chain triglycerides (group 4) as the source of fat for an additional 2 weeks. Rats in groups 5 and 6 were fed fish oil-ethanol and fish oil-dextrose, respectively, for 8 weeks. Liver samples were analyzed for histopathology, lipid peroxidation, and levels of messenger RNA (mRNA) for Cox-2 and TNF-alpha. Concentrations of endotoxin were determined in plasma. The most severe inflammation and fibrosis were detected in groups 1 and 5, as were the highest levels of endotoxin, lipid peroxidation, and mRNA for Cox-2 and TNF-alpha. After ethanol was discontinued, there was minimal histological improvement in group 2 but near normalization of the histology, including regression of fibrosis, in groups 3 and 4. Histological improvement was associated with decreased levels of endotoxin, lipid peroxidation, and reduced expression of Cox-2 and TNF-alpha. The data indicate that a diet enriched in saturated fatty acids (groups 3 and 4) effectively reverses alcohol-induced liver injury, including fibrosis. The therapeutic effects of saturated fatty acids may be explained, at least in part, by reduced endotoxemia and lipid peroxidation, which in turn result in decreased levels of TNF-alpha and Cox-2.
Lipoproteins protect against endotoxemia and TNF-alpha:
Eur Heart J. 1993 Dec;14 Suppl K:125-9.
The protective effect of serum lipoproteins against bacterial lipopolysaccharide.
Read TE, Harris HW, Grunfeld C, Feingold KR, Kane JP, Rapp JH.
Lipoproteins bind and inactivate bacterial endotoxin, both in vitro and in vivo. Both cholesterol ester-rich and TG-rich lipoproteins, and TG-rich lipid emulsions can prevent death in mice when pre-incubated with a lethal dose of endotoxin before intraperitoneal administration. Chylomicrons can also prevent death when given intravenously after endotoxin in rats. The metabolic fate of lipoprotein-bound endotoxin appears to be directed by the lipoprotein particle. When administered with chylomicrons, the plasma clearance and hepatic uptake of endotoxin are enhanced. Endotoxin is shunted preferentially to hepatocytes and away from hepatic macrophages, thereby increasing endotoxin excretion [corrected] in bile. The survival benefit and alterations in metabolism afforded by chylomicrons correlate with a reduction in peak serum levels of tumour necrosis factor (TNF), providing a possible mechanism by which lipoproteins protect against endotoxin-induced death. These findings suggest a possible role for lipoproteins or lipid emulsions in the body’s defence against endotoxaemia.
Dairy lowers TNF-alpha in the overweight:
Am J Clin Nutr January 2010 vol. 91 no. 1 16-22
Effects of dairy compared with soy on oxidative and inflammatory stress in overweight and obese subjects
Michael B Zemel, Xiaocun Sun, Teresa Sobhani, and Beth Wilson
Background: We recently showed that calcitriol increases oxidative and inflammatory stress; moreover, inhibition of calcitriol with high-calcium diets decreased both adipose tissue and systemic oxidative and inflammatory stress in obese mice, whereas dairy exerted a greater effect. However, these findings may be confounded by concomitant changes in adiposity.
Objective: The objective of this study was to evaluate the acute effects of a dairy-rich diet on oxidative and inflammatory stress in overweight and obese subjects in the absence of adiposity changes.
Design: Twenty subjects (10 obese, 10 overweight) participated in a blinded, randomized, crossover study of dairy- compared with soy-supplemented eucaloric diets. Two 28-d dietary periods were separated by a 28-d washout period. Inflammatory and oxidative stress biomarkers were measured on days 0, 7, and 28 of each dietary period.
Results: The dairy-supplemented diet resulted in significant suppression of oxidative stress (plasma malondialdehyde, 22%; 8-isoprostane-F2α, 12%; P < 0.0005) and lower inflammatory markers (tumor necrosis factor-α, 15%, P < 0.002; interleukin-6, 13%, P < 0.01; monocyte chemoattractant protein-1, 10%, P < 0.0006) and increased adiponectin (20%, P < 0.002), whereas the soy exerted no significant effect. These effects were evident by day 7 of treatment and increased in magnitude at the end of the 28-d treatment periods. There were no significant differences in response to treatment between overweight and obese subjects for any variable studied.
Conclusion: An increase in dairy food intake produces significant and substantial suppression of the oxidative and inflammatory stress associated with overweight and obesity. This trial was registered at clinicaltrials.gov as NCT00686426.
Am J Clin Nutr August 2011 vol. 94 no. 2 422-430
Dairy attentuates oxidative and inflammatory stress in metabolic syndrome
Renée A Stancliffe, Teresa Thorpe, and Michael B Zemel
Background: Oxidative and inflammatory stress are elevated in obesity and are further augmented in metabolic syndrome. We showed previously that dairy components suppress the adipocyte- and macrophage-mediated generation of reactive oxygen species and inflammatory cytokines and systemic oxidative and inflammatory biomarkers in obesity.
Objective: The objective of this study was to determine the early (7 d) and sustained (4 and 12 wk) effects of adequate-dairy (AD) compared with low-dairy (LD) diets in subjects with metabolic syndrome.
Design: Forty overweight and obese adults with metabolic syndrome were randomly assigned to receive AD (3.5 daily servings) or LD (<0.5 daily servings) weight-maintenance diets for 12 wk. Oxidative and inflammatory biomarkers were assessed at 0, 1, 4, and 12 wk as primary outcomes; body weight and composition were measured at 0, 4, and 12 wk as secondary outcomes.
Results: AD decreased malondialdehyde and oxidized LDL at 7 d (35% and 11%, respectively; P < 0.01), with further decreases by 12 wk. Inflammatory markers were suppressed with intake of AD, with decreases in tumor necrosis factor-α at 7 d and further reductions through 12 wk (35%; P < 0.05); decreases in interleukin-6 (21%; P < 0.02) and monocyte chemoattractant protein 1 (14% decrease at 4 wk, 24% decrease at 12 wk; P < 0.05); and a corresponding 55% increase in adiponectin at 12 wk (P < 0.01). LD exerted no effect on oxidative or inflammatory markers. Diet had no effect on body weight; however, AD significantly reduced waist circumference and trunk fat (P < 0.01 for both), and LD exerted no effect.
Conclusion: An increase in dairy intake attenuates oxidative and inflammatory stress in metabolic syndrome. This trial was registered at clinicaltrials.gov as NCT01266330.



 latest posts")